This disorder operates in silence. There are no visible marks or clear symptoms, only prolonged bleeding when it should cease. For millions worldwide living with hemophilia, this often-invisible reality influences everything from childhood activities to menstruation, as well as considerations for surgery.
Each year on April 17, World Hemophilia Day draws attention to this frequently overlooked condition. The date was selected by the World Federation of Haemophilia (WFH) to urge governments and policymakers toward achievable goals: improved treatment, enhanced access, and better care. The necessity for this push decades after its inception highlights how hemophilia often remains sidelined.
At its essence, hemophilia is a clotting disorder characterized by the absence or insufficiency of specific proteins known as Factor VIII or Factor IX, which signal the blood to halt after an injury. The result can be life-threatening internal bleeding even into muscles or joints. This condition is rare, hereditary, and widely misunderstood.
Genetically, hemophilia is linked to the X chromosome, making diagnosis more common among men. A boy with a carrier mother has a 50% probability of inheriting the condition. However, the belief that hemophilia “only affects men” dismisses the reality of many women who carry the gene, facing significant risks including heavy menstrual cycles, complications during childbirth, and unexpected bleeding.
World Hemophilia Day aims to address this erasure, focusing on both policy and public perception.
The Daily Reality: Pain, Precautions, and the Constant Risk of Bleeding Episodes
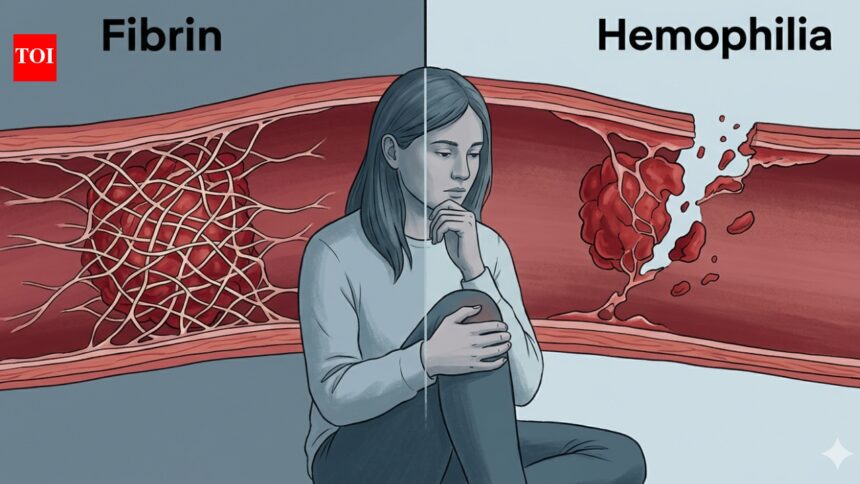
Many associate hemophilia purely with external cuts. However, the actual experience is far graver. When an individual sustains an injury, the body first constricts the damaged vessel to slow down bleeding. Next, platelets cluster to form a temporary seal, followed by clotting proteins that weave a strong fibrin mesh over the plug to ensure healing.
For those with hemophilia, the initial steps often function normally; the vessels constrict and platelets gather. The issue arises with the formation of the fibrin clot, which may either fail to form or be too weak to last, leading to continued or recurring bleeding. Contrary to common belief, individuals with hemophilia typically do not face lethal outcomes from minor cuts; the true hazard lies deeper within the body.
Internal bleeding transforms hemophilia into a life-altering condition. Blood that pools in joints or muscles can result in severe damage, particularly in the knees, elbows, and ankles. Over time, repeated internal bleeding—even with treatment—can degrade cartilage and create premature osteoarthritis.
Ordinary situations can trigger these bleeds—a bump on the knee during a commute or an elbow striking a doorframe—often unnoticed by people without hemophilia. Some bleeds occur spontaneously, without any apparent trigger, posing urgent medical risks.
Timing is critical; unlike surface injuries that can be bandaged, internal bleeding necessitates immediate treatment with clotting factors to prevent further damage. Delays can lead to increased pain, joint deterioration, and prolonged recovery.
“Patients suffering from hemophilia face multiple daily challenges,” notes Dr. Geetika Jassal, Medical Spokesperson at Cryoviva Life Sciences. “The constant risk of spontaneous bleeding into joints can cause chronic pain, swelling, and reduced mobility over time. Managing the condition demands regular infusions of clotting factors, frequent hospital visits, and strict adherence to treatment schedules, which can be taxing both physically and financially.”
From Diagnosis to Delay: Why Early Detection Remains a Global Challenge
Despite being documented for centuries, hemophilia is still frequently misdiagnosed. Its severity varies—ranging from severe to moderate to mild. Each category exhibits different behaviors, meaning mild cases may evade notice for years or even decades.
Individuals with severe hemophilia might exhibit symptoms early, such as unexplained bruising or swollen joints. Conversely, those with mild hemophilia often manage everyday scrapes without significant issues, revealing their blood’s insufficiency only under stressful conditions like surgery or childbirth.
As such, diagnosis often arrives as a shock for many.
The Family History Gap
Many families opt for newborn testing when hemophilia is present in the lineage, leading to early detection in several cases. However, about one in three babies diagnosed with hemophilia carry new genetic mutations not present in either parent, leading to sudden diagnoses without prior warning.
As a result, a considerable number of individuals with hemophilia remain undiagnosed until symptoms manifest unexpectedly.
“Early signs of hemophilia can be subtle and may be mistaken for normal childhood injuries, such as frequent bruising or prolonged bleeding from minor cuts. Many parents might dismiss these signals as routine, which delays diagnosis,” Dr. Jassal adds.
The Women Who Get Missed
Furthermore, women, who are often overlooked, face unique challenges. The perception of hemophilia as a male-exclusive disorder impacts patient care. Women carriers may experience heavy menstrual cycles or prolonged healing times, but without relevant inquiry or awareness, their symptoms can be misdiagnosed.
The official diagnosis frequently follows years of having their concerns minimized.
What Detection Actually Looks Like
When hemophilia is suspected, testing typically involves a blood examination assessing clotting and subsequent factor assays to identify specific deficiencies. While the medical protocols exist, the challenge lies in whether practitioners think to investigate.
This gap is especially prominent in low-income regions, where access to specialized care can be limited, but it also exists in well-resourced health systems, impacting mild cases or unrecognized women.
Early detection is crucial. It allows families to prepare, enables timely medical interventions, and fosters a deeper understanding of the body before crises arise. While medical advancements have progressed, the awareness surrounding hemophilia continues to lag behind.
“Early diagnosis is essential to prevent irreversible joint damage and life-threatening bleeding episodes. Initiating prophylactic treatment drastically improves quality of life; however, gaps in awareness continue to pose significant concerns,” Dr. Jassal explains.
From Plasma Bags to Precision Medicine: The Evolution of Hemophilia Treatment
The first effective treatments for hemophilia emerged in 1964, with options limited to basic products such as cryoprecipitate derived from plasma. For most, obtaining treatment involved significant logistical challenges.
Since that time, treatment options have evolved dramatically, transitioning from plasma-derived products to recombinant clotting factor concentrates. Newer technologies include extended half-life therapies that minimize the frequency of infusions. Some treatments can now be administered subcutaneously, easing the burden on patients and especially benefiting children or those living in remote areas.
Recent developments include emicizumab, a bispecific antibody differing from traditional factor replacement. It is administered under the skin, allows for less frequent dosage, and does not lead to inhibitor development seen in some patients using conventional factor concentrates—an advancement unimaginable a generation ago.
At the forefront of treatment is gene therapy, requiring only a single intervention that prompts the liver to produce the essential clotting factors. The FDA approved two gene therapies for hemophilia B, Hemgenix in 2022 and Beqvez in 2024, and one for severe hemophilia A, marking a significant shift in treatment paradigms.
“Recent studies are exploring advanced approaches such as gene therapy and stem cell-based strategies to address the underlying causes rather than merely managing symptoms. Stem cell research is still largely experimental but shows promise,” Dr. Jassal notes.
Where Does India Stand?
India has the second-highest prevalence of hemophilia globally, with approximately 136,000 cases. While the nation has recently conducted its first in-human gene therapy trial, many patients continue to rely on rudimentary methods for bleed management.
This disparity highlights a core issue in hemophilia care in India: cutting-edge research coexists with significant underserved populations.
The Insurance and Money Problem
Within India’s health economy, hemophilia is often neglected—too rare for sustained policy focus, too costly for adequate treatment. Most affected families find private insurance prohibitively expensive. Given hemophilia’s classification as a low-volume, high-cost syndrome, insurers have little incentive to provide comprehensive coverage.
This creates a scenario where financial constraints dictate access to treatment. Many patients rely on basic methods such as RICE (rest, ice, compression, elevation) alongside adjunct medications and episodic use of products like fresh frozen plasma or cryoprecipitate. These coping mechanisms are not genuine treatments but rather stopgap measures.
“Access to specialized centers remains limited in India, with care primarily revolving around clotting factor replacement and emerging therapies when available,” Dr. Jassal states.
Overall, the healthcare framework continues to treat a chronic condition as if it were a series of acute emergencies. The consequences of untreated hemophilia—hospitalizations, surgeries, long-term disabilities, and lost productivity—burden families and healthcare systems alike, underscoring the need for early and comprehensive care.